What part of the elbow is affected?
The bones of the elbow are the humerus (the upper arm bone), the ulna (the larger bone of the forearm, on the opposite side of the thumb), and the radius (the smaller bone of the forearm on the same side as the thumb).
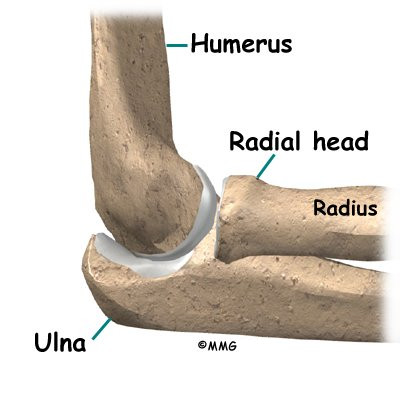
The elbow itself is essentially a hinge joint, meaning it bends and straightens like a hinge. But there is a second joint where the end of the radius (the radial head) meets the humerus. This joint is complicated because the radius has to rotate so that you can turn your hand palm up and palm down. At the same time, it has to slide against the end of the humerus as the elbow bends and straightens. The joint is even more complex because the radius has to slide against the ulna as it rotates the wrist as well. As a result, the end of the radius at the elbow is shaped like a smooth knob with a cup at the end to fit on the end of the humerus. The edges are also smooth where it glides against the ulna.
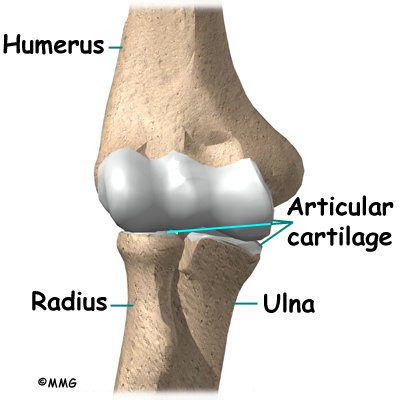
Articular cartilage is the material that covers the ends of the bones of any joint. Articular cartilage can be up to one-quarter of an inch thick in the large, weight-bearing joints. It is a bit thinner in joints such as the elbow, which don't support weight. Articular cartilage is white, shiny, and has a rubbery consistency. It is slippery, which allows the joint surfaces to slide against one another without causing any damage. In the elbow, articular cartilage covers the end of the humerus, the end of the radius, and the end of the ulna.
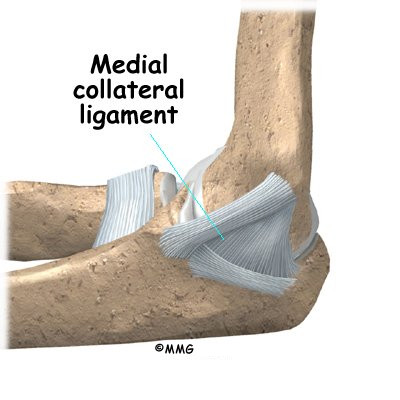
There are several important ligaments in the elbow. Ligaments are soft tissue structures that connect bones to bones. The ligaments around a joint usually combine together to form a joint capsule. A joint capsule is a watertight sac that surrounds a joint and contains lubricating fluid called synovial fluid.
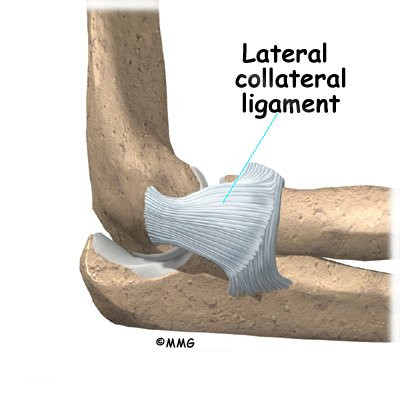
In the elbow, two of the most important ligaments are themedial collateral ligament and the lateral collateral ligament. The medial collateral is on the inside edge of the elbow, and the lateral collateral is on the outside edge. Together these two ligaments connect the humerus to the ulna and keep it tightly in place as it slides through the groove at the end of the humerus. These ligaments are the main source of stability for the elbow. They can be torn when there is an injury to or dislocation of the elbow. If they do not heal correctly the elbow can be too loose, or unstable.
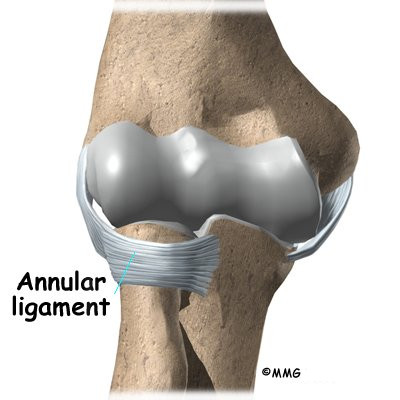
There is also an important ligament called the annular ligament that wraps around the radial head and holds it tight against the ulna. The word annular means ring-shaped. The annular ligament forms a ring around the radial head as it holds it in place. This ligament can be torn when the entire elbow or just the radial head is dislocated.
Causes
What can cause this condition?
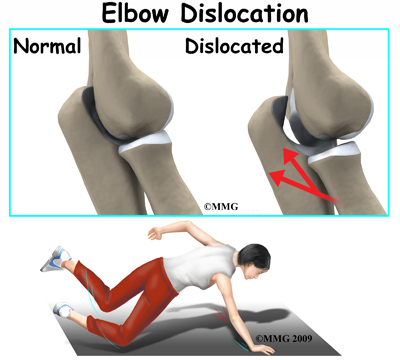
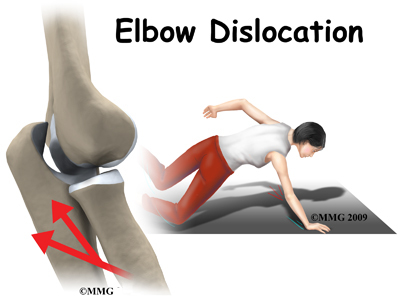
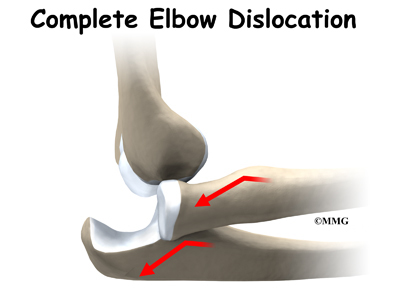
Elbow dislocation is often the result of trauma. The most common trauma resulting in an elbow dislocation is a fall onto an outstretched hand and arm. When the hand hits the ground, the force is transmitted through the forearm to the elbow. This force pushes the elbow out of its socket.
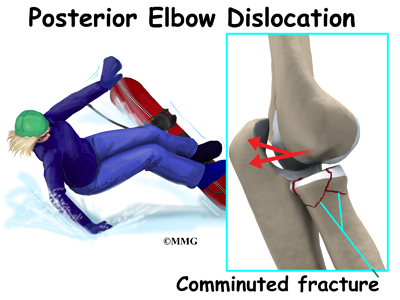 This can also result in a fracture/dislocation. About half of all elbow dislocations in teens and young adults occur as a result of a sports activity. The most common elbow dislocations are associated with sports such as gymnastics, cycling, rollerblading, or skateboarding.
This can also result in a fracture/dislocation. About half of all elbow dislocations in teens and young adults occur as a result of a sports activity. The most common elbow dislocations are associated with sports such as gymnastics, cycling, rollerblading, or skateboarding.
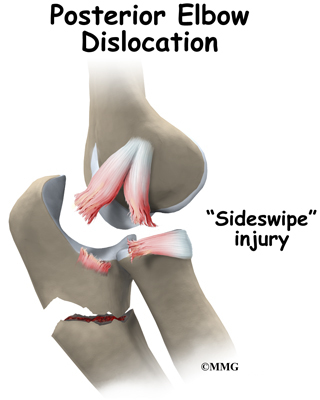
Dislocation can also occur from a sideswipe injury. This type of injury occurs when the driver of an automobile has the elbow out the open window during a car accident. The force of the impact causes a severe fracture-dislocation of the elbow.
Symptoms
What does this condition feel like?
If the elbow is fully dislocated, it will look out of joint. There may be dimples or indentations of the skin over the dislocation where the bones have shifted position. Pain can be intense until the arm is relocated. The pain is often relieved immediately after the joint is put back in place. There may be some residual tenderness around the joint.
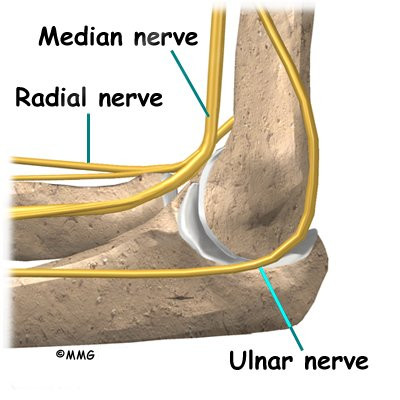
If ligaments or other soft tissues are torn, there can be swelling and bruising around the elbow. Bruising is not immediately obvious but appears several days after the injury. Injury to any of the three nerves that cross the elbow (median, ulnar, radial nerves) can cause neurologic symptoms such as numbness, tingling, and/or weakness of the forearm, wrist, and hand. If a bone fracture is also involved the fracture can cut or damage a nerve causing temporary or permanent paralysis.
Pain and an inability to straighten the elbow or pain when turning the hand the palm up (supination) is typical. There is often tenderness along the lateral aspect of the elbow (side of the elbow away from the body).
Diagnosis
How do doctors diagnose elbow dislocation?
The history and physical examination are probably the most important tools the physician uses to guide his or her diagnosis. Moving the elbow passively is painful, especially extension and supination. The doctor will check for any signs of injury to the nerves or blood vessels.
X-ray is the best way to look for dislocation or fracture-dislocation.
After the joint is relocated, other imaging studies may be ordered to look for damage to the joint cartilage, bone, ligaments, and other soft tissues. If bone detail is difficult to identify on an X-ray, a computed tomography (CT) scan may be done. If it is important to evaluate the ligaments, a magnetic resonance image (MRI) can be helpful.
Treatment
What treatment options are available?
Nonsurgical Treatment
It is possible for the elbow to relocate by itself. This is more likely when there is a subluxation, rather than a complete dislocation. Sometimes the elbow can be reduced or put back in place by a trained medical person applying a quick motion to the forearm. There are several different methods used for manual (closed) reduction. Closed reduction refers to the fact that the elbow can be put back in joint without surgery. An open incision is not needed.
Manual reduction can be done in an emergency on site (e.g., at an athletic event or car accident) by a trained medical person but usually the procedure is done in a clinic or hospital setting. You would be given medications first to help with the pain.
Surgery
If there is too much swelling, it may be necessary to delay surgery for a few days up to a week. The elbow will be reduced right away and the arm immobilized while waiting for the swelling to subside.
If there has been damage to the bones and/or ligaments, surgery may be needed to restore alignment and function. The type of surgery depends on the extent of the damage. Wires, pins, or even an external fixation device may be needed to hold everything together until healing occurs.
Rehabilitation
What should I expect after treatment?
Nonsurgical Rehabilitation
Simple elbow dislocations heal well with few (if any) problems. You may notice a slight loss of elbow motion, especially when trying to straighten the arm. This should not affect your overall motion and function. X-rays may be taken while the elbow heals. This will show if the bones of the elbow joint are healing in a reduced position with good alignment.
The arm may be immobilized for 10 to 14 days to allow the ligament to heal. Gentle range of motion may be allowed during that time but you should rely on your physician to advise you. Type of activities and movements allowed are determined according to the type of injury that's present.
After immobilization, physical therapy may begin. The goal is to restore normal motion, joint proprioception (sense of position), and motor control. The program will progress to include strengthening.
Rehabilitation for the athlete includes sport-specific training is part of the rehab program. Your physical therapist will guide you through this process. Most athletes can resume sports participation three to six weeks after an elbow dislocation. The timing of return to sports depends on the type of sport (e.g., throwing sports may require a longer rehab). Dislocation of the dominant hand may require longer rehab before full motion and strength are restored.
Some athletes continue to wear a protective splint and/or use taping to stabilize the joint during the transition back into action. This can help protect the joint during motion and activity during the final phase of healing.
It's best to avoid any further traction on the elbow until healing has occurred. Pulling a heavy door open, carrying a heavy purse, or lifting a heavy backpack are a few examples of activities and movements that put a traction force through the elbow. These kinds of movements should be avoided until healing occurs.
After Surgery
Post-operative immobilization is often required, especially for complex injuries. This could be a cast, dynamic splint, or postoperative range-of-motion (ROM) brace. The adjustable ROM brace is used to improve elbow motion gradually while allowing soft tissue healing. It helps minimize scar tissue formation and may contribute to fewer complications (such as arthritis) later on.
After immobilization, physical therapy may begin. The goals are the same as for conservative (nonoperative) care: restore normal motion, joint proprioception (sense of position), and motor control. The program will progress to include strengthening. Rely on your doctor and therapist to guide you through the healing process.
As in conservative care, some athletes continue to wear a protective splint and/or use taping to stabilize the joint during the transition back into action. This can help protect the joint during motion and activity during the final phase of healing.
It's best to avoid any further traction on the elbow until healing has occurred. Pulling a heavy door open, carrying a heavy purse, or lifting a heavy backpack are a few examples of activities and movements that put a traction force through the elbow. These kinds of movements should be avoided until healing occurs. Your doctor and/or therapist will advise you as you progress through the healing process.
Scar tissue can cause a stiff elbow. Recurrent dislocation is also possible. If either of these problems develops, additional reconstructive surgery may be needed. For some patients, arthritis is a long-term result of elbow injury. This is more likely if there is a history of recurrent elbow dislocations.