A Patient’s Guide to Piriformis Syndrome
Introduction
Pain in the buttock that radiates down the leg is commonly called sciatica. The most common cause for sciatica is irritation of the spinal nerves in or near the lumbar spine. Sometimes the nerve irritation is not in the spine but further down the leg. One possible cause of sciatica is piriformis syndrome. Piriformis syndrome can be painful, but it is seldom dangerous and rarely leads to the need for surgery. Most people with this condition can reduce the pain and manage the problem with simple methods, such as physical therapy.
This guide will help you understand
- how the problem develops
- how doctors diagnose the condition
- what treatment options are available
Anatomy
What parts of the body are involved?
The lower lumbar spinal nerves leave the spine and join to form the sciatic nerve. The sciatic nerve leaves the pelvis through an opening called the sciatic notch.
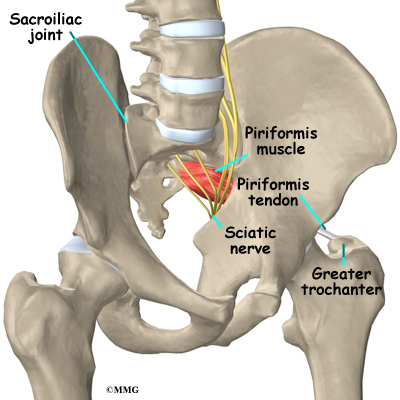
The piriformis muscle begins inside the pelvis. It connects to the sacrum, the triangular shaped bone that sits between the pelvic bones at the base of the spine. The connection of the sacrum to the pelvis bones forms the sacroiliac joint. There is one sacroiliac joint on the left and one on the right of the low back. The other end of the piriformis muscle connects by a tendon to the greater trochanter, the bump of bone on the top side of your hip.

The piriformis muscle is one of the external rotators of the hip and leg. This means that as the muscle works, it helps to turn the foot and leg outward. Problems in the piriformis muscle can cause problems with the sciatic nerve. This is because the sciatic nerve runs under (and sometimes through) the piriformis muscle on its way out of the pelvis. The piriformis muscle can squeeze and irritate the sciatic nerve in this area, leading to the symptoms of sciatica.
Related Document: A Patient’s Guide to Lumbar Spine Anatomy
Causes
What causes this problem?

The symptoms of sciatica come from irritation of the sciatic nerve. It’s still a mystery why the piriformis muscle sometimes starts to irritate the sciatic nerve. Many doctors think that the condition begins when the piriformis muscle goes into spasm and tightens
against the sciatic nerve, squeezing the nerve against the bone of the pelvis.
In some cases, the muscle may be injured due to a fall onto the buttock. Bleeding in and around the piriformis muscle forms a hematoma. A hematoma describes the blood that has pooled in that area.
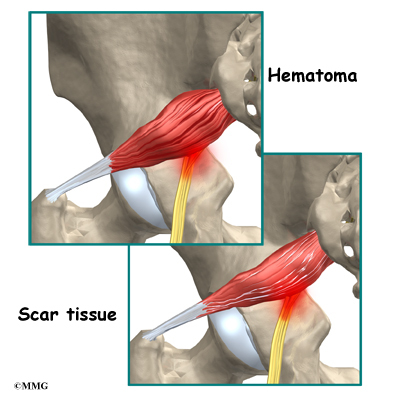
The piriformis muscle begins to swell and put pressure on the sciatic nerve. Soon the hematoma dissolves, but the muscle goes into spasm.
The sciatic nerve stays irritated and continues to be a problem. Eventually the muscle heals, but some of the muscle fibers inside the piriformis muscle are replaced by scar tissue. Scar tissue is not nearly as flexible and elastic as normal muscle tissue. The
piriformis muscle can tighten up and put constant pressure against the sciatic nerve.
Symptoms
What does the condition feel like?
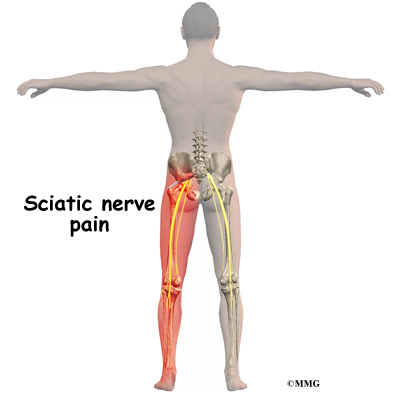
Piriformis syndrome commonly causes pain that radiates down the back of the leg. The pain may be felt only on one side, though it is sometimes felt on both sides. The pain can radiate down the leg all the way to the foot and may be confused for a herniated disc in the lumbar spine. Changes in sensation and weakness in the leg or foot are rare. Some people say they feel a sensation of vague tingling down the leg.
Sitting may be difficult. Usually people with piriformis syndrome do not like to sit. When they do sit down, they tend to sit with the sore side buttock tilted up rather than sitting flat in the chair.
Diagnosis
How do doctors diagnose the problem?
Diagnosis begins with a complete history and physical exam. Your doctor will ask questions about your symptoms and how the pain is affecting your daily activities. Your doctor will also want to know what positions or activities make your symptoms worse or better. You will be asked about any injuries in the past and about any other medical problems you might have such as any arthritis that runs in the family.
Next the doctor examines you by checking your posture, how you walk, and where your pain is located. Your doctor checks to see which back movements cause pain or other symptoms.
Your skin sensation, muscle strength, and reflexes are also tested because it is difficult to distinguish pain coming from the sacroiliac joint from pain coming from other spine conditions.
If there is any question whether you might have an infection or some type of arthritis affecting multiple joints, laboratory tests may be ordered. You may need to have blood drawn and give a urine sample to send to the laboratory for special tests.
X-rays are commonly ordered of both the low back and pelvis. X-rays can give your doctor an idea about how much wear and tear has developed in the sacroiliac joint. X- rays of the lumbar spine and hips are also helpful to rule out problems in these areas that may look and act like sacroiliac joint problems.
Other radiological tests may also be useful. A magnetic resonance imaging (MRI) scan can be used to look at the lumbar spine and pelvis in much more detail and rule out other conditions in the area conditions. The MRI scan uses magnetic waves rather than X-rays and shows a very detailed picture of the soft tissues of the body.
A special type of MRI scan called neurography is being used more frequently to look at nerves. This uses a regular MRI scanner, but the computer settings are set to look for areas of irritation along a nerve. This may change the way doctors use the MRI to diagnose nerve problems such as piriformis syndrome, thoracic outlet syndrome, and carpal tunnel syndrome.
A bone scan is useful to see how the skeleton is reacting to any type of “stress,” such as an injury, an infection, or inflammation from arthritis. Chemical “tracers” are injected into your blood stream. The tracers then show up on special spine X- rays. The tracers collect in areas where the bone tissue is reacting strongly to some type of stress to the skeleton, such as arthritis and infection of the sacroiliac joint.
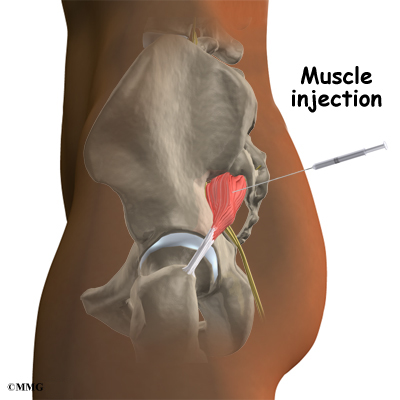
The most accurate way to tell if the piriformis muscle is the cause of pain is with a diagnostic injection into the muscle. The muscle is deep inside the buttock, so the injection requires X-ray guidance with a fluoroscope, a CT scanner, or an open MRI machine. Once the needle is placed in the muscle, an anesthetic can be injected into the muscle to paralyze the piriformis muscle. If the pain goes away after the injection, your doctor can be reasonably sure that the pain you are feel is from piriformis syndrome.
Treatment
What treatment options are available?
Nonsurgical Treatment
Doctors often begin by prescribing nonsurgical treatment for piriformis syndrome. In some cases, doctors simply monitor their patients’ condition to see if symptoms improve. Anti-inflammatory medications, such as ibuprofen and naproxen, are commonly used to treat the pain and inflammation caused by the irritation on the nerve. Acetaminophen (for example Tylenol®) can be used to treat the pain but will not control the inflammation.
You’ll probably work with a physical therapist. After evaluating your condition, the therapist uses treatments to ease spasm and pain in the piriformis muscle. Exercises, particularly stretching exercises, are given to try and relieve irritation on the sciatic nerve.
If you still have pain after trying these treatments, your doctor may suggest injections.The main use of injections is to see if your pain is from piriformis syndrome. An injection of local anesthetic such as lidocaine can be injected into the muscle to temporarily relax it. This loosens up the muscle and reduces the irritation on the sciatic nerve. Other medications have also been injected into the piriformis muscle. Cortisone, for example, may be mixed with the anesthetic medication to reduce the inflammation on the sciatic nerve. Cortisone is a potent anti-inflammatory medication that is commonly used both in pill form and in injections to treat inflammation.
Related Document: A Patient’s Guide to Piriformis Muscle Injections
Botulism injection therapy (also known as Botox® injections) can be used to actually paralyze the piriformis muscle. This makes the muscle relax, which helps take pressure off the sciatic nerve. The effect of the Botox® injection isn’t permanent; it generally only lasts a few months. In the meantime, however, it is hoped that a stretching program can be used to fix the problem. In other words, when the injection wears off, the muscle may have been stretched enough so that the symptoms do not return.
Surgery
Surgery may be considered but usually only as a last resort. There are two procedures in use. The first is to cut the piriformis tendon where it attaches on the greater trochanter (the bump on the side of your hip). The other method is to cut through the piriformis muscle to take pressure off the sciatic nerve.
These procedures are usually done on an outpatient basis, meaning that you will be able to go home the same day as the surgery. In some cases, you may need to stay in the hospital for one night. Both procedures can be done under general anesthesia or under a spinal type of anesthetic.
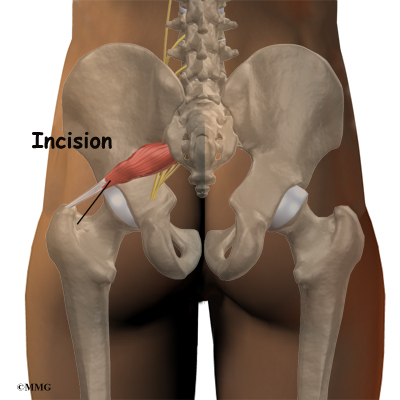
The surgeon begins by making a small incision, usually about three inches long, in the buttock. The fibers of the gluteus maximus, the largest buttock muscle, are split. This gives the surgeon a way to see deep into the buttock and locate the piriformis muscle. When the piriformis muscle and tendon can be seen, the surgeon then cuts (releases) the tendon where it connects to the greater trochanter.
If more room is needed to release the pressure on the nerve, a portion of the piriformis muscle may be removed.
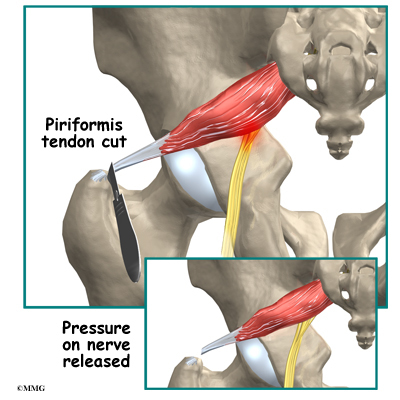
This usually doesn’t cause problems with strength because there are several much stronger muscles that help turn the leg outward.
Rehabilitation
What should I expect as I recover?
Nonsurgical Rehabilitation
Most patients with piriformis syndrome work with a physical therapist. Plan to attend physical therapy sessions two to three times each week for six to eight weeks.
Your therapist begins by evaluating your condition. This includes attention to the low back, as well as the sacroiliac and hip joints.
Physical therapy treatments for piriformis syndrome often begin with heat applications. Heat is used to help the piriformis muscle relax, easing spasm and pain. Your physical therapist may place a hot pack over your buttocks muscle.
Ultrasound is another treatment choice that can be set for deep heating in the buttock area. Ultrasound uses high frequency sound waves that are directed through the skin. The deep heating effect of ultrasound is ideal for preparing the piriformis muscle for hands-
on forms of treatment and for getting the muscle to stretch out.
Hands-on treatments such as deep massage and specialized forms of soft-tissue mobilization may be used initially. Your therapist may also position your hip and leg in a way that helps to relax nerve signals to the piriformis.
The keystone treatment for piriformis treatment is stretching. Stretching is especially effective following heat and hands on treatments. Your therapist will position you in ways that help you get a good stretch on the piriformis muscle. Along with the stretches
you’ll do in the clinic, you’ll be shown several ways to stretch the muscle on your own. You need to do your stretches every few hours. Be gentle and cautious as you stretch to avoid overdoing it.
As your symptoms ease, your therapist will gradually advance your program to include posture training, muscle strengthening, and general conditioning.
After Surgery
Your surgeon may prescribe physical therapy after surgery for piriformis syndrome. You’ll probably only need to attend sessions for four to six weeks. Expect full recovery to take up to three months.
During therapy after surgery, your therapist may use treatments such as heat or ice, electrical stimulation, massage, and ultrasound to help calm pain and muscle spasm. Then you’ll begin learning how to move safely with the least strain on the healing area.
As the rehabilitation program evolves, you’ll begin doing more challenging exercises. The goal is to safely advance strength and function.
As the therapy sessions come to an end, your therapist helps you get back to the activities you enjoy. Ideally, you’ll be able to resume normal activities. You may need guidance on which activities are safe or how to change the way they go about their activities.
When treatment is well under way, regular visits to your therapist’s office will end. Your therapist will continue to be a resource. But you’ll be in charge of doing your exercises as part of an ongoing home program.