A Patient’s Guide to Osgood-Schlatter Lesion of the Knee
Introduction
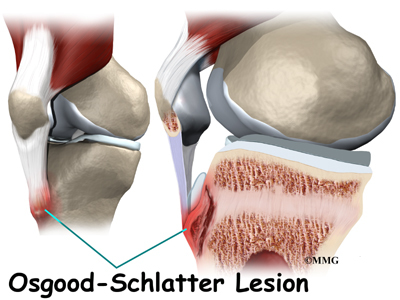
An Osgood-Schlatter lesion involves pain and swelling in the small bump of bone on the front of the tibia (shinbone), right below the kneecap. It occurs in children and adolescents. The problem affects the area where bone growth occurs. Too much stress on the growing bone causes the pain and swelling. The pain often worsens with activity and eases with rest. Fortunately, the condition is not serious. It is usually only temporary.
The condition is the most frequent cause of knee pain in children between the ages of 10 and 15. The problem used to happen mostly in boys. But with more girls playing sports, boys and girls are now affected equally. Because girls’ skeletons begin to mature earlier than boys, girls tend to have this condition when they are one to two years younger than boys. Kids who play sports have this condition 20 percent more often than nonathletes. And the lesion seems to run in families; when one child is affected, there’s a 30 percent chance a sibling will have it, too.
This guide will help you understand
- why the condition develops
- how doctors diagnose the condition
- what treatment options are available
Anatomy
What part of the knee is affected?
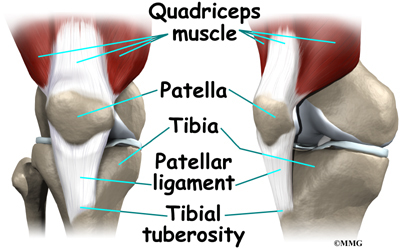
The Osgood-Schlatter lesion affects the tibial tuberosity. The tibial tuberosity is the bump on the top of the tibia (shinbone) where the patellar tendon connects. Tendons connect muscles to bones. The patellar tendon stretches over the top of the patella (kneecap). The patellar tendon connects the large quadriceps muscle on the front of the thigh to the tibial tuberosity. As the quadriceps muscle works, it pulls on the patellar tendon and extends (straightens) the knee joint.

A small bursa sometimes develops where the patellar tendon meets the tibial tuberosity. A bursa is a normal structure that often forms in areas where friction occurs, such as between muscles, tendons, and bones. A bursa is a thin sac of tissue filled with fluid. The fluid lubricates the area and reduces friction.
Related Document: A Patient’s Guide to Knee Anatomy
Causes
How did this problem develop?
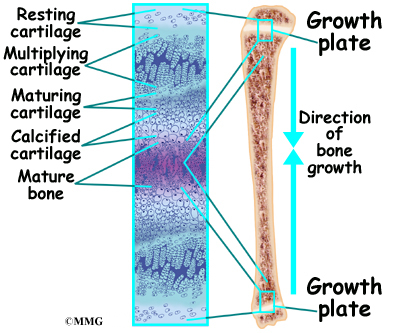
Osgood-Schlatter lesions fit in a category of bone development disorders known as osteochondroses. (Osteo means bone, and chondro means cartilage.) In normal development, specialized bone growth centers (called growth plates) change over time from cartilage to bone. The growth centers expand and finally unite. This is how bones grow in length and width. Bone growth centers are located throughout the body.
Children with bone development problems in one area are likely to develop similar problems elsewhere. For example, among young athletes with growth plate problems in the back of the heel (Sever’s syndrome), about two-thirds also develop an Osgood-Schlatter lesion. Children who have an Osgood-Schlatter lesion also have a small chance of problems at the top of the patellar tendon, where it attaches to the bottom tip of the kneecap. This condition is known as Sinding-Larsen-Johansson disorder.
Related Document: A Patient’s Guide to Sever’s Syndrome
Related Document: A Patient’s Guide to Jumper’s Knee in Children and Adolescents
The main cause of Osgood-Schlatter lesions is too much tension in the patellar tendon. The tension can come from overuse from sports activity and from growth spurts. Usually both happen together. Both put extra stress on the tibial tuberosity.
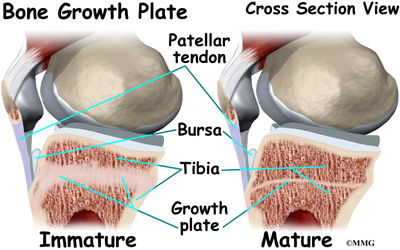
During growth spurts, the tendon may not be able to keep up with the growth of the lower leg. The tendon becomes too short. It constantly pulls at the tibial tuberosity. Tension from sports activity comes from overuse. When the quadriceps muscle on the front of the thigh works, it pulls on the patellar tendon. The tendon in turn pulls on the tibial tuberosity. If the tension is too great and occurs too often while the bone is developing, it can pull the growth area of the tibial tuberosity away from the growth area of the shinbone.
The bump forms because the separated growth plates keep growing and expanding. The area between the bone fragments fills in with new tissue, either cartilage or bone. The new tissue causes the tibial tuberosity to become enlarged and painful.

Another possible cause of Osgood-Schlatter lesions is abnormal alignment in the legs. Kids who are knock-kneed or flat-footed seem to be most prone to the condition. These postures put a sharper angle between the quadriceps muscle and the patellar tendon. This angle is called the Q-angle. A large Q-angle puts more tension on the bone growth plate of the tibial tuberosity, increasing the chances for an Osgood-Schlatter lesion to develop. A high-riding patella, called patella alta, is also thought to contribute to development of Osgood-Schlatter lesions.
Symptoms
What does an Osgood-Schlatter lesion feel like?
In an Osgood-Schlatter lesion, the tibial tuberosity will probably be enlarged and painful. It hurts when bumped. It also hurts when pressure is put on it, such as when kneeling. Activities like running, jumping, climbing, and kicking may hurt because of the tension of the patellar tendon pulling on the tibial tuberosity.
Symptoms generally go away gradually over a period of one to two years. However, the condition may leave a permanent, painless bump below the knee. The area may always be tender. Many adults who had a lesion as a child still have pain when kneeling on that knee.
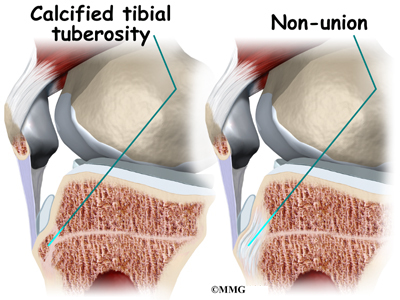
Complications can occur if the area between the bone fragments fills in with cartilage rather than bone. Normally, the bone growth plates join together with solid bone in between. If cartilage fills in the space, the condition is called a nonunion.
Diagnosis
How do doctors diagnose the condition?
A doctor can usually make the diagnosis from the history and physical examination. The doctor will want to know the child’s age and activity level, and whether there are any siblings who’ve had an Osgood-Schlatter lesion.
The doctor will press on and around the patella and patellar tendon to see if there is any tenderness. The doctor will compare the sore knee and the healthy knee. The doctor may also ask the patient to straighten the knee against resistance. This makes the quadriceps muscle work, putting tension on the patellar tendon. Pain during this test can help the doctor make the diagnosis of an Osgood-Schlatter lesion.
The history and physical examination are usually the only tests necessary, but sometimes an X-ray is ordered. A knee X-ray may show a raised area of irregular bone in the tibial tuberosity. Most often it will show swelling in the soft tissues in front of the tibial tuberosity. In more severe cases, the X-ray may show small bony fragments that are separated from the rest of the tibial tuberosity.

An X-ray is necessary if the tibial tuberosity hurts after an injury such as a fall. In this case, the X-ray will help the doctor see if the tibial tuberosity fractured as a result of the trauma.
Treatment
What can be done for the problem?
Nonsurgical Treatment
The passing of time may be all that is needed. It takes one to two years for the bone growth plates of the tibial tuberosity to grow together and form one solid bone. When this occurs, symptoms usually go away completely.
In some cases, the patient may need to stop sport activities for a short period. This gets the pain and inflammation under control. Usually patients don’t need to avoid sports for a long time. It is unlikely that the bone will completely separate, so not all athletes need to completely avoid sports.

The doctor may prescribe anti-inflammatory medicine to help reduce swelling. Physical therapists might use ice, heat, or ultrasound to control inflammation and pain. A variety of pads, straps, and sleeves are available that can help keep pain to a minimum. For example, wearing a knee pad cushions the sore area while kneeling.
As symptoms ease, the physical therapist works on flexibility, strength, and muscle balance in the knee. Posture exercises can help improve knee alignment. The therapist may also design special shoe inserts, called orthotics, to support flat feet or to correct knock-kneed posture.
Cortisone injections are commonly used to control pain and inflammation in other types of injuries. However, a cortisone injection is usually not appropriate for Osgood-Schlatter lesions. Cortisone injections haven’t shown consistently good results for this condition. There is also a high risk that the cortisone will cause the patellar tendon to rupture.
Severe pain and problems may require a knee brace or cast for up to six weeks. The goal is to stop the knee from moving so that inflammation and pain go away.
Surgery
Surgery is not considered unless bone growth is complete and symptoms are still bothersome despite nonsurgical treatments. Even then, surgery for an Osgood-Schlatter lesion is rarely recommended.
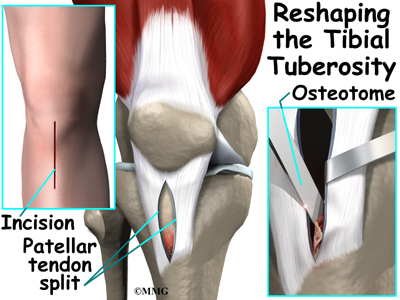
When surgery is needed, the usual operation involves removing the raised area of the tibial tuberosity, the bursa, and irritated tissue nearby. The surgeon makes a small incision down the front of the lower knee, just over the tibial tuberosity. The patellar tendon is split in half. Retractors are used to pull the skin and the patellar tendon apart. This makes it easy for the surgeon to see and work on the tibial tuberosity. The surgeon uses an osteotome to cut away the raised area of the tibial tuberosity. Care is taken while removing the bursa and nearby tissue.
The retractors are removed. The cut edges of the patellar tendon are brought together. Scar tissue eventually binds the edges back together. To complete the operation, the surgeon stitches up the skin.
Rehabilitation
What can be expected from treatment?
Nonsurgical Rehabilitation
With nonsurgical rehabilitation, the goal is to reduce pain and inflammation. These measures can help. However, most Osgood-Schlatter lesions still get better over time, as the bones mature.
Some doctors have their patients work with a physical therapist. Therapists work on the possible causes of the problem. For example, flexibility exercises for the hamstring and quadriceps muscles can help reduce tension in the patellar tendon where it attaches to the tibial tuberosity. Orthotics are sometimes issued to put the leg and knee in good alignment. Strengthening exercises to improve muscle balance can help the kneecap move correctly during activity. Therapists work with athletes to improve form and to reduce knee strain during sports.
When symptoms are especially bad, patients may be instructed to avoid any activity that makes their pain worse, including sports. In severe cases, bracing or casting may be needed for up to six weeks.
After Surgery
After surgery, daily activities can be resumed gradually. The knee should be propped up routinely during the day to help reduce swelling and throbbing. Medicines should be taken exactly as prescribed by the surgeon.
The surgeon may recommend using crutches or a cane for awhile. Vigorous activities and exercise should be avoided for six weeks after surgery. Athletes should not take part in high-level sports for two to three months. Some surgeons have their patients attend physical therapy after surgery.